

Introduction: The role of the immune system and the microenvironment in Hodgkin Lymphoma (HL) has been well established. However, little is known about the effects of treatment on the immune cells in the peripheral blood or the frequency of tumor specific T cell responses to non-EBV HL specific antigens in pediatric and adolescent patients with HL. The goal of this project was to evaluate whether patients had increased tumor specific cytotoxic T cell responses and a pro-inflammatory cytokine milieu after treatment compared to at diagnosis.
Methods: Peripheral blood samples were collected at diagnosis(pre) and following completion of treatment (post) from newly diagnosed high risk classical HL patients ages ≥2 to 22 years enrolled on a Children's Oncology Group sponsored Phase 3 clinical trial AHOD1331 randomizing to therapy containing the anti-CD30 immunoconjugate Brentuximab(Bv-AVEPC) vs. standard chemotherapy (ABVE-PC) (NCT02166463). Peripheral blood mononuclear cells (PBMC) and plasma were isolated using Ficoll Density gradient and analyzed in 206 patients to date. Pre and post plasma samples from 175 patients were tested for Th1/Th2 cytokines by Luminex assay. Tumor specific T cell responses at pre and post treatment have been tested in 64 of the 175 patients. Briefly, non-adherent T cells were stimulated ex vivo with autologous dendritic cells pulsed with HL specific pepmixes for the non-EBV tumor associated antigens (TAA) MAGEA4, PRAME and Survivin and expanded for a week in the presence of cytokines. TAA specificity was then tested using Interferon-γ ELISPOT assay. Immunophenotyping of the T cell subsets and the exhaustion marker profile was performed by flow cytometry in 49 patients with available PBMCs at both time points. Changes in cytokine levels pre versus post treatment were compared in univariate and multivariate analyses including the following variables: age at diagnosis, gender, stage, B symptoms, bulky disease and EBER status.
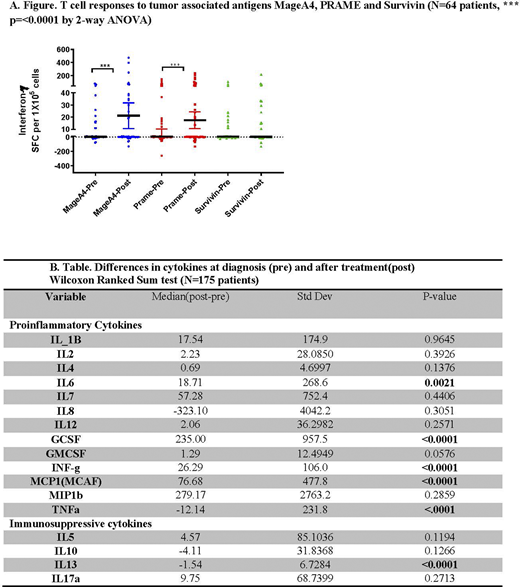
Results: There was no difference in patient characteristics between the entire study cohort (n=587) and patients analyzed (n=206). There was a significant decrease in peripheral blood helper T cells (CD3+CD4+) and an increase in cytotoxic T cells (CD3+/CD8+) after treatment compared to at diagnosis (n=49 patients; p<0.0001). There was no difference in the expression of the exhaustion markers PD1, TIM3 and LAG3 at diagnosis versus post treatment. In vivo T cell responses to at least one of the three tumor associated antigens MAGEA4, PRAME and Survivin were detected in 41/64 (61%) patients at diagnosis and 39/64 (60%) patients post treatment. There was a significant increase in T cell responses to MAGEA4 and PRAME (p<0.0001, See Fig A) after treatment as compared to pre-treatment. Cytokine profiling demonstrated a significant reduction in the immunosuppressive cytokine IL-13 (p<0.0001) and a significant increase in pro-inflammatory cytokines IL-6, Interferon-γ, GCSF, MCAF (CCL22) but surprisingly, there was a decrease in TNFα (all p<0.001) post treatment (n=175 patients, See Table B). In multivariable models bulk and/or EBER status at diagnosis were significantly associated with (p<0.05) the change between post and pre treatment in some cytokine profile measurements (IL2, IL4, IL5, IL7, IL17a, GCSF, GMCSF and TNFα)
Conclusions: T cell responses to tumor associated antigens can be detected in patients with HL at diagnosis and after treatment. Increased T cell responses to MAGE4 and PRAME post therapy suggests that recovery post anti-HL treatment can promote tumor antigen specific T cell immunity in vivo. Further, reduced IL-13 and increased Interferon-γ following treatment suggest a favorable milieu for T cell expansion. Correlations between immune responses and clinical outcomes will be performed once outcome data are available. The impact of Bv will be evaluated by comparing the differences of the immune responses by treatment arm. Our results will help identify immune markers of response that can guide future immunotherapies for HL.
Bollard:Mana Therapeutics: Other: IP.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal